
Pathogenesis of Penile Squamous Cell Carcinoma: Molecular Update and Systematic Review

 ,
,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methodology
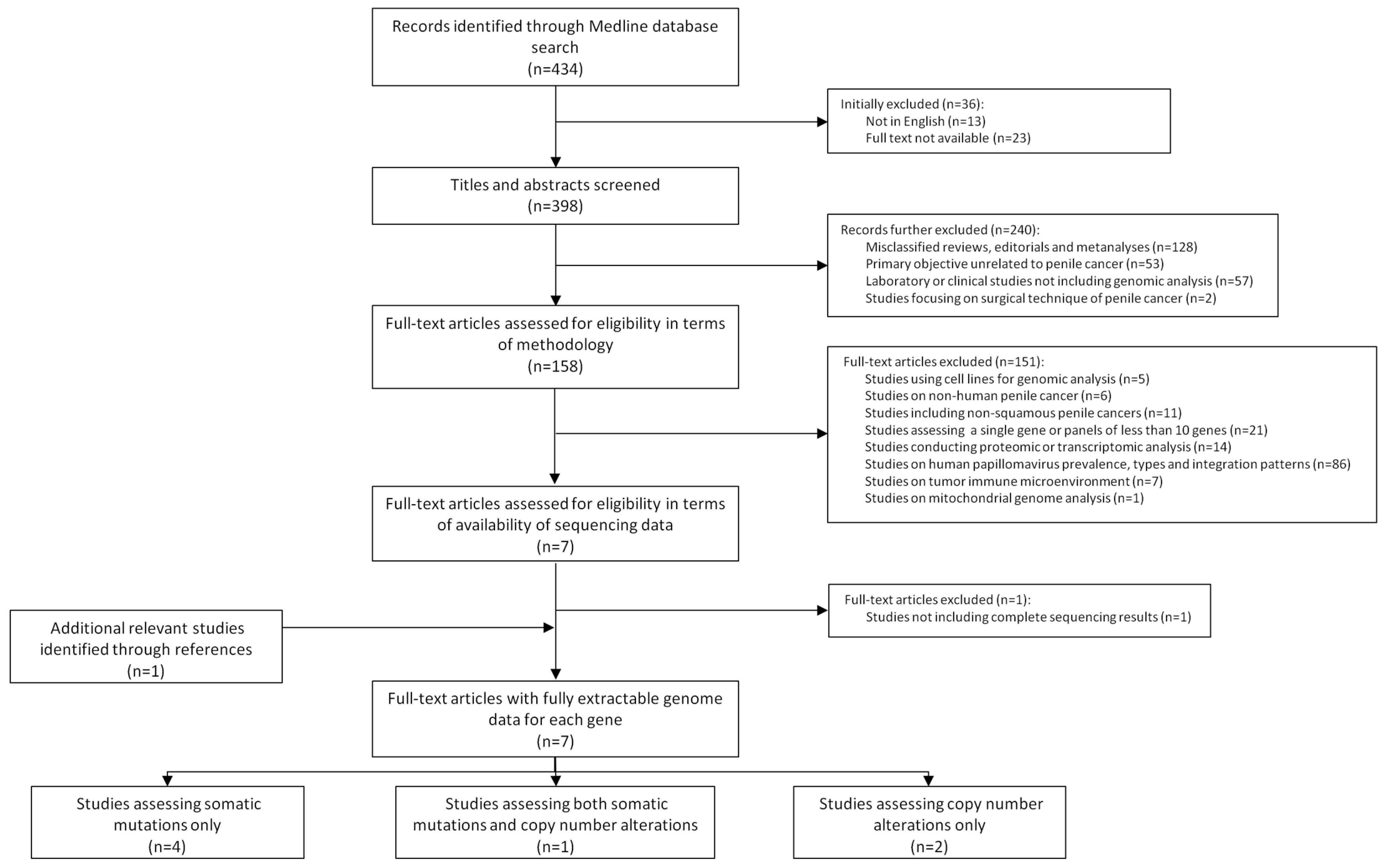
2.1. Literature Revision and Criteria of Selection
2.2. Study Selection
2.3. Methodological Features of the Studies
3. Results
3.1. Somatic Mutations
3.2. Copy Number Variations
3.3. Relationship with HPV Status
3.4. Mutational Signatures and Signaling Pathways in PSCC
3.5. Prognostic Implications of Mutations and Copy Number Alterations in PSCC
3.6. Potential Therapeutic Targets to Treat PSCC
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Cardona, C.E.M.; García-Perdomo, H.A. Incidence of penile cancer worldwide: Systematic review and meta-analysis. Rev. Panam. Salud Pública 2017, 41, e117. [Google Scholar] [CrossRef] [Green Version]
- Emmanuel, A.; Nettleton, J.; Watkin, N.; Berney, D.M. The molecular pathogenesis of penile carcinoma—current developments and understanding. Virchows Arch. 2019, 475, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Crispen, P.L.; Mydlo, J.H. Penile Intraepithelial Neoplasia and Other Premalignant Lesions of the Penis. Urol. Clin. N. Am. 2010, 37, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Chaux, A.; Pfannl, R.; Lloveras, B.; Alejo, M.; Clavero, O.; Lezcano, C.; Muñoz, N.; José, F.X.B.; Bosch, X.; Hernández-Pérez, M.; et al. Distinctive Association of p16INK4a Overexpression with Penile Intraepithelial Neoplasia Depicting Warty and/or Basaloid Features: A Study of 141 Cases Evaluating a New Nomenclature. Am. J. Surg. Pathol. 2010, 34, 385–392. [Google Scholar] [CrossRef]
- Jouhi, L.; Hagström, J.; Atula, T.; Mäkitie, A. Is p16 an adequate surrogate for human papillomavirus status determination? Curr. Opin. Otolaryngol. Head Neck Surg. 2017, 25, 108–112. [Google Scholar] [CrossRef]
- Alemany, L.; Cubilla, A.; Halec, G.; Kasamatsu, E.; Quirós, B.; Masferrer, E.; Tous, S.; Lloveras, B.; Hernández-Suarez, G.; Lonsdale, R.; et al. Role of Human Papillomavirus in Penile Carcinomas Worldwide. Eur. Urol. 2016, 69, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Canete-Portillo, S.; Sanchez, D.F.; Cubilla, A.L. Pathology of Invasive and Intraepithelial Penile Neoplasia. Eur. Urol. Focus 2019, 5, 713–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cubilla, A.L.; Lloveras, B.; Alejo, M.; Clavero, O.; Chaux, A.; Kasamatsu, E.; Monfulleda, N.; Tous, S.; Alemany, L.; Klaustermeier, J.; et al. Value of p16(INK)4(a) in the pathology of invasive penile squamous cell carcinomas: A report of 202 cases. Am. J. Surg. Pathol. 2011, 35, 253–261. [Google Scholar] [CrossRef]
- Chaux, A.; Pfannl, R.; Rodríguez, I.M.; Barreto, J.E.; Velazquez, E.F.; Lezcano, C.; Piris, A.; Netto, G.J.; Cubilla, A.L. Distinctive immunohistochemical profile of penile intraepithelial lesions: A study of 74 cases. Am. J. Surg. Pathol. 2011, 35, 553–562. [Google Scholar] [CrossRef]
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs—Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Kidd, L.C.; Chaing, S.; Chipollini, J.; Giuliano, A.R.; Spiess, P.E.; Sharma, P. Relationship between human papillomavirus and penile cancer-implications for prevention and treatment. Transl. Androl. Urol. 2017, 6, 791–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hakenberg, O.W.; Dräger, D.L.; Erbersdobler, A.; Naumann, C.M.; Jünemann, K.P.; Protzel, C. The Diagnosis and Treatment of Penile Cancer. Dtsch. Aerzteblatt Int. 2018, 115, 646. [Google Scholar] [CrossRef] [PubMed]
- Stecca, C.E.; Alt, M.; Jiang, D.M.; Chung, P.; Crook, J.M.; Kulkarni, G.S.; Sridhar, S.S. Recent Advances in the Management of Penile Cancer: A Contemporary Review of the Literature. Oncol. Ther. 2021, 9, 21–39. [Google Scholar] [CrossRef]
- McGregor, B.A.; Sonpavde, G.P. New insights into the molecular profile of penile squamous cell carcinoma. Clin. Cancer Res. 2021, 27, 2375–2377. [Google Scholar] [CrossRef] [PubMed]
- Jacob, J.; Ferry, E.; Gay, L.; Elvin, J.A.; Vergilio, J.A.; Ramkissoon, S.; Severson, E.; Necchi, A.; Killian, J.K.; Ali, S.M.; et al. Comparative Genomic Profiling of Refractory and Metastatic Penile and Nonpenile Cutaneous Squamous Cell Carcinoma: Implications for Selection of Systemic Therapy. J. Urol. 2019, 201, 541–548. [Google Scholar] [CrossRef]
- Vanthoor, J.; Vos, G.; Albersen, M. Penile cancer: Potential target for immunotherapy? World J. Urol. 2020, 39, 1405–1411. [Google Scholar] [CrossRef] [PubMed]
- Carreras-Dieguez, N.; Guerrero, J.; Rodrigo-Calvo, M.; Ribera-Cortada, I.; Trias, I.; Jares, P.; López Del Campo, R.; Saco, A.; Munmany, M.; Marimon, L.; et al. Molecular Landscape of Vulvar Squamous Cell Carcinoma. Int. J. Mol. Sci. 2021, 22, 7069. [Google Scholar] [CrossRef]
- Feber, A.; Worth, D.C.; Chakravarthy, A.; de Winter, P.; Shah, K.; Arya, M.; Saqib, M.; Nigam, R.; Malone, P.R.; Tan, W.S.; et al. CSN1 Somatic Mutations in Penile Squamous Cell Carcinoma. Cancer Res. 2016, 76, 4720–4727. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wang, K.; Chen, Y.; Zhou, J.; Liang, Y.; Yang, X.; Li, X.; Cao, Y.; Wang, D.; Luo, L.; et al. Mutational landscape of penile squamous cell carcinoma in a Chinese population. Int. J. Cancer 2019, 145, 1280–1289. [Google Scholar] [CrossRef]
- Chahoud, J.; Gleber-Netto, F.O.; McCormick, B.Z.; Rao, P.; Lu, X.; Guo, M.; Morgan, M.B.; Chu, R.A.; Martinez-Ferrer, M.; Eterovic, A.K.; et al. Whole-exome Sequencing in Penile Squamous Cell Carcinoma Uncovers Novel Prognostic Categorization and Drug Targets Similar to Head and Neck Squamous Cell Carcinoma. Clin. Cancer Res. 2021, 27, 2560–2570. [Google Scholar] [CrossRef]
- Ferrándiz-Pulido, C.; Hernández-Losa, J.; Masferrer, E.; Vivancos, A.; Somoza, R.; Marés, R.; Valverde, C.; Salvador, C.; Placer, J.; Morote, J.; et al. Identification of somatic gene mutations in penile squamous cell carcinoma. Genes Chromosomes Cancer 2015, 54, 629–637. [Google Scholar] [CrossRef]
- Macedo, J.; Silva, E.; Nogueira, L.; Coelho, R.; da Silva, J.; Dos Santos, A.; Teixeira-Júnior, A.A.; Belfort, M.; Silva, G.; Khayat, A.; et al. Genomic profiling reveals the pivotal role of hrHPV driving copy number and gene expression alterations, including mRNA downregulation of TP53 and RB1 in penile cancer. Mol. Carcinog. 2020, 59, 604–617. [Google Scholar] [CrossRef] [PubMed]
- Yongbo, Y.; Chengwen, G.; Yuanbin, C.; Wang, M.; Zhang, J.; Ma, X.; Liu, S.; Yuan, H.; Li, Z.; Niu, H. Copy Number Analysis Reveal Genetic Risks of Penile Cancer. Front. Oncol. 2020, 10, 596261. [Google Scholar] [CrossRef]
- McDaniel, A.S.; Hovelson, D.H.; Cani, A.K.; Liu, C.-J.; Zhai, Y.; Zhang, Y.; Weizer, A.Z.; Mehra, R.; Feng, F.Y.; Alva, A.S.; et al. Genomic Profiling of Penile Squamous Cell Carcinoma Reveals New Opportunities for Targeted Therapy. Cancer Res. 2015, 75, 5219–5227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebhandl, S.; Huemer, M.; Greil, R.; Geisberger, R. AID/APOBEC deaminases and cancer. Oncoscience 2015, 2, 320–333. [Google Scholar] [CrossRef] [Green Version]
- Peng, Z.; Gong, Y.; Liang, X. Role of FAT1 in health and disease. Oncol. Lett. 2021, 21. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Ye, X.; Liu, Y.; Wei, W.; Wang, Z.; Wang, L.; Ye, X.; Liu, Y.; Wei, W.; Wang, Z. Aberrant regulation of FBW7 in cancer. Oncotarget 2014, 5, 2000–2015. [Google Scholar] [CrossRef] [Green Version]
- Ciriello, G.; Miller, M.L.; Aksoy, B.A.; Senbabaoglu, Y.; Schultz, N.; Sander, C. Emerging landscape of oncogenic signatures across human cancers. Nat. Genet. 2013, 45, 1127–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, Y.; Tang, X.; Liu, M. Tumor-suppressor gene NBPF1 inhibits invasion and PI3K/mTOR signaling in cervical cancer cells. Oncol. Res. 2016, 23, 13–20. [Google Scholar] [CrossRef]
- Rehmani, H.S.; Issaeva, N. EGFR in head and neck squamous cell carcinoma: Exploring possibilities of novel drug combinations. Ann. Transl. Med. 2020, 8, 813. [Google Scholar] [CrossRef]
- Busso-Lopes, A.F.; Marchi, F.A.; Kuasne, H.; Scapulatempo-Neto, C.; Trindade-Filho, J.C.S.; de Jesus, C.M.N.; Lopes, A.; Guimarães, G.C.; Rogatto, S.R. Genomic profiling of human penile carcinoma predicts worse prognosis and survival. Cancer Prev. Res. 2015, 8, 149–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuasne, H.; Barros-Filho, M.C.; Busso-Lopes, A.; Marchi, F.A.; Pinheiro, M.; Muñoz, J.J.M.; Scapulatempo-Neto, C.; Faria, E.F.; Guimarães, G.C.; Lopes, A.; et al. Integrative miRNA and mRNA analysis in penile carcinomas reveals markers and pathways with potential clinical impact. Oncotarget 2017, 8, 15294–15306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peter, M.; Rosty, C.; Couturier, J.; Radvanyi, F.; Teshima, H.; Sastre-Garau, X. MYC activation associated with the integration of HPV DNA at the MYC locus in genital tumors. Oncogene 2006, 25, 5985–5993. [Google Scholar] [CrossRef] [Green Version]
- Allen-Petersen, B.L.; Sears, R.C. Mission Possible: Advances in MYC Therapeutic Targeting in Cancer. BioDrugs 2019, 33, 539–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adimonye, A.; Stankiewicz, E.; Kudahetti, S.; Trevisan, G.; Tinwell, B.; Corbishley, C.; Lu, Y.J.; Watkin, N.; Berney, D. Analysis of the PI3K-AKT-mTOR pathway in penile cancer: Evaluation of a therapeutically targetable pathway. Oncotarget 2018, 9, 16074–16086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wykosky, J.; Fenton, T.; Furnari, F.; Cavenee, W.K. Therapeutic targeting of epidermal growth factor receptor in human cancer: Successes and limitations. Chin. J. Cancer 2011, 30, 5. [Google Scholar] [CrossRef] [PubMed]
- Cordani, M.; Oppici, E.; Dando, I.; Butturini, E.; Dalla Pozza, E.; Nadal-Serrano, M.; Oliver, J.; Roca, P.; Mariotto, S.; Cellini, B.; et al. Mutant p53 proteins counteract autophagic mechanism sensitizing cancer cells to mTOR inhibition. Mol. Oncol. 2016, 10, 1008–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, P.A.; Huang, C.; Li, Q.; Kazi, S.A.; Byers, L.A.; Wang, J.; Johnson, F.M.; Frederick, M.J. NOTCH1 Signaling in Head and Neck Squamous Cell Carcinoma. Cells 2020, 9, 2677. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author, Year and Reference | Country | Number of Patients | Number of Samples | Characteristics of the Sample | HPV Test | HPV Prevalence | Type of Genomic Analysis | Gene Panel | Number of Targeted Genes | Platform/Sequencing Depth (for NGS Studies) |
|---|---|---|---|---|---|---|---|---|---|---|
| Studies assessing only somatic mutations (n = 4) | ||||||||||
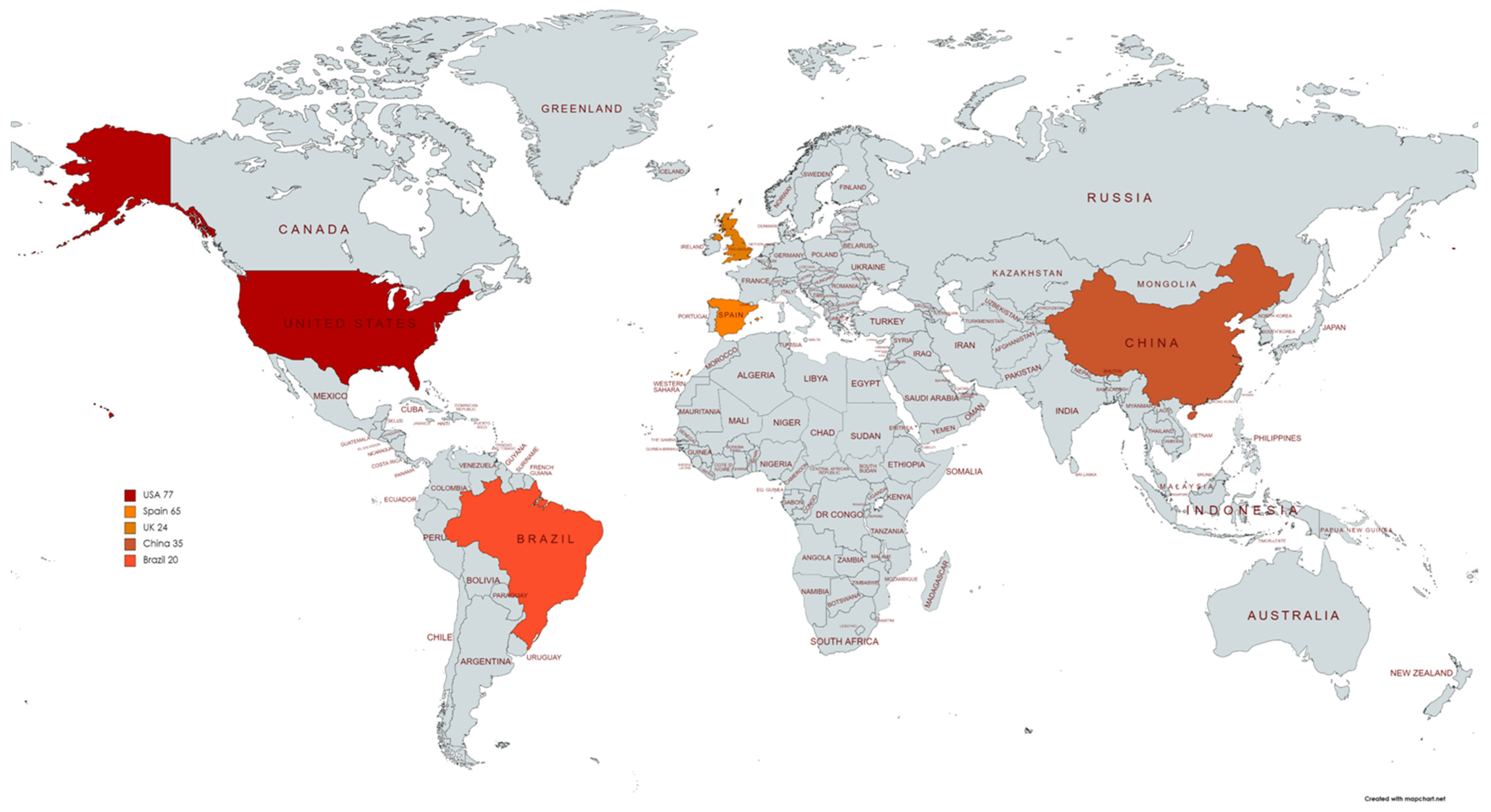
| Ferrándiz-Pulido (2015) | Spain | 65 | 65 | FFPE | Unspecified PCR and p16 | 28% | Targeted mass spectrometry sequencing | Oncocarta mutation panel v1.0 | 19 | N/A |
| Feber (2016) | UK | 24 | 24 | Not specified | Unspecified qPCR | 37% | Whole exome sequencing | N/A | Whole exome | Hi-Seq 2000/60x |
| Wang (2019) | China | 30 | 30 | Fresh frozen | PCR-reverse dot blot assay | 20% | Whole exome sequencing | N/A | Whole exome | Hi-Seq 2500/130x |
| Chahoud (2021) | USA | 34 | 34 | Fresh frozen | Cobas HPV assay and p16 | 29% | Whole exome sequencing | N/A | Whole exome | Hi-Seq 4000/141x |
| Studies assessing both somatic mutations and copy number variations (n = 1) | ||||||||||
| McDaniel (2015) | USA | 43 | 60 * | FFPE | GP5+/GP6+My09/11 and p16 | 12% | Multiplex-based targeted NGS | Oncomine Comprehensive Panel | 126 | PGM/535x |
| Studies assessing only copy number variations (n = 2) | ||||||||||
| Macedo (2020) | Brazil | 20 | 20 | FFPE and fresh frozen | My09/My11 | 96% | aCGH; TaqMan copy number assay in the genes of PI3K/AKT pathway | N/A | N/A | N/A |
| Yongbo (2020) | China | 35 | 35 | Fresh frozen | PCR-reverse dot blot assay | 20% ** | Whole exome sequencing | N/A | Whole exome | Hi-Seq2500/120x |
| Gene | Studies Evaluating the Gene | Studies Identifying Alterations in the Gene | Total Number of PSCC Assessed | Number of PSCC with Alterations in the Gene | Overall Frequency (%) | Frequency Range (%) |
|---|---|---|---|---|---|---|
| Genes identified in more than one study | ||||||
| TP53 | 4 | 4 | 148 | 48 | 32.4 | 10–48 |
| NOTCH1 | 4 | 4 | 148 | 26 | 17.6 | 7–44 |
| PIK3CA | 4 | 4 | 189 | 25 | 13.2 | 9–21 |
| HRAS | 4 | 4 | 179 | 20 | 11.2 | 6–17 |
| CDKN2A | 3 | 3 | 118 | 30 | 25.4 | 4–32 |
| FAT1 | 3 | 3 | 88 | 22 | 25.0 | 13–35 |
| CASP8 | 3 | 3 | 88 | 15 | 17.0 | 13–24 |
| FBXW7 | 3 | 3 | 118 | 13 | 11.0 | 8–15 |
| NFE2L2 | 3 | 3 | 114 | 12 | 10.5 | 8–12 |
| TTN | 2 | 2 | 64 | 14 | 21.9 | 10–32 |
| MUC17 | 2 | 2 | 58 | 8 | 13.8 | 13–15 |
| FLG | 2 | 2 | 54 | 7 | 12.9 | 10–17 |
| EP300 | 2 | 2 | 58 | 6 | 10.3 | 4–15 |
| KRAS | 2 | 2 | 125 | 8 | 6.4 | 3–9 |
| KIT | 2 | 2 | 89 | 4 | 4.5 | 3–8 |
| BRAF | 2 | 2 | 125 | 4 | 3.0 | 3–3 |
| Genes identified in a single study | ||||||
| NBPF1 | 1 | 1 | 24 | 13 | 54.2 | N/A |
| MLL3 | 1 | 1 | 24 | 9 | 37.5 | N/A |
| HLA-B | 1 | 1 | 24 | 5 | 20.8 | N/A |
| MUC4 | 1 | 1 | 34 | 7 | 20.6 | N/A |
| DNAH6 | 1 | 1 | 34 | 6 | 17.6 | N/A |
| GXYLT1 | 1 | 1 | 24 | 4 | 16.7 | N/A |
| AHNAK2 | 1 | 1 | 34 | 5 | 14.7 | N/A |
| LAMA1 | 1 | 1 | 34 | 5 | 14.7 | N/A |
| MUC2 | 1 | 1 | 34 | 5 | 14.7 | N/A |
| XRP2 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| NSD1 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| IL7R | 1 | 1 | 24 | 3 | 12.5 | N/A |
| DNAH12 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| WASF3 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| TSC1 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| SETDB1 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| NF1 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| COL5A3 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| CHD4 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| ANK3 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| ALK | 1 | 1 | 24 | 3 | 12.5 | N/A |
| ZNF462 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| ZBTB5 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| NID1 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| IQGAP2 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| INSR | 1 | 1 | 24 | 3 | 12.5 | N/A |
| HEXA | 1 | 1 | 24 | 3 | 12.5 | N/A |
| CNTLN | 1 | 1 | 24 | 3 | 12.5 | N/A |
| PFAS | 1 | 1 | 24 | 3 | 12.5 | N/A |
| PAPLN | 1 | 1 | 24 | 3 | 12.5 | N/A |
| CENPJ | 1 | 1 | 24 | 3 | 12.5 | N/A |
| C2CD3 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| ATP10D | 1 | 1 | 24 | 3 | 12.5 | N/A |
| ASXL1 | 1 | 1 | 24 | 3 | 12.5 | N/A |
| HHAT | 1 | 1 | 24 | 3 | 12.5 | N/A |
| AK302511 | 1 | 1 | 34 | 4 | 11.8 | N/A |
| ARPP21 | 1 | 1 | 34 | 4 | 11.8 | N/A |
| BIRC6 | 1 | 1 | 34 | 4 | 11.8 | N/A |
| CACNA1C | 1 | 1 | 34 | 4 | 11.8 | N/A |
| CSPG4 | 1 | 1 | 34 | 4 | 11.8 | N/A |
| FAT4 | 1 | 1 | 34 | 4 | 11.8 | N/A |
| FHAD1 | 1 | 1 | 34 | 4 | 11.8 | N/A |
| FRG1 | 1 | 1 | 34 | 4 | 11.8 | N/A |
| FRY | 1 | 1 | 34 | 4 | 11.8 | N/A |
| FSIP2 | 1 | 1 | 34 | 4 | 11.8 | N/A |
| GRIN2B | 1 | 1 | 34 | 4 | 11.8 | N/A |
| KMT2B | 1 | 1 | 34 | 4 | 11.8 | N/A |
| MYO188 | 1 | 1 | 34 | 4 | 11.8 | N/A |
| PDE4DIP | 1 | 1 | 34 | 4 | 11.8 | N/A |
| PKD1 | 1 | 1 | 34 | 4 | 11.8 | N/A |
| SLITRK2 | 1 | 1 | 30 | 3 | 10.0 | N/A |
| TRRAP | 1 | 1 | 30 | 3 | 10.0 | N/A |
| CCDC168 | 1 | 1 | 30 | 3 | 10.0 | N/A |
| SACS | 1 | 1 | 24 | 2 | 8.3 | N/A |
| NUP210L | 1 | 1 | 24 | 2 | 8.3 | N/A |
| MGA | 1 | 1 | 24 | 2 | 8.3 | N/A |
| USP31 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| TM9SF1 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| TGM1 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| SNX19 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| SMG6 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| SLC7A6OS | 1 | 1 | 24 | 2 | 8.3 | N/A |
| PITPNM2 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| PIGT | 1 | 1 | 24 | 2 | 8.3 | N/A |
| NCF2 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| MTHFR | 1 | 1 | 24 | 2 | 8.3 | N/A |
| IQCG | 1 | 1 | 24 | 2 | 8.3 | N/A |
| INADL | 1 | 1 | 24 | 2 | 8.3 | N/A |
| GPS1 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| FAM72D | 1 | 1 | 24 | 2 | 8.3 | N/A |
| DFNA5 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| CX3CR1 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| CREB3L4 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| CPNE1 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| CHPT1 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| BRCA1 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| ZFHX3 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| TXNDC8 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| TNFRSF14 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| TGFBR2 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| TET2 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| TDRD10 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| SNX25 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| SELP | 1 | 1 | 24 | 2 | 8.3 | N/A |
| PRDM1 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| OTUD7A | 1 | 1 | 24 | 2 | 8.3 | N/A |
| NTN4 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| NCOR1 | 1 | 1 | 24 | 2 | 8.3 | N/A |
| HLA-A | 1 | 1 | 24 | 2 | 8.3 | N/A |
| CREBBP | 1 | 1 | 24 | 2 | 8.3 | N/A |
| BRE | 1 | 1 | 24 | 2 | 8.3 | N/A |
| ATM | 1 | 1 | 24 | 2 | 8.3 | N/A |
| PDGFA | 1 | 1 | 65 | 3 | 4.6 | N/A |
| ZRANB3 | 1 | 1 | 24 | 1 | 4.2 | N/A |
| ZNF180 | 1 | 1 | 24 | 1 | 4.2 | N/A |
| TIMM17A | 1 | 1 | 24 | 1 | 4.2 | N/A |
| STK19 | 1 | 1 | 24 | 1 | 4.2 | N/A |
| SPEN | 1 | 1 | 24 | 1 | 4.2 | N/A |
| OR52N1 | 1 | 1 | 24 | 1 | 4.2 | N/A |
| OR4A16 | 1 | 1 | 24 | 1 | 4.2 | N/A |
| MYOCD | 1 | 1 | 24 | 1 | 4.2 | N/A |
| MORC4 | 1 | 1 | 24 | 1 | 4.2 | N/A |
| MICALCL | 1 | 1 | 24 | 1 | 4.2 | N/A |
| ITPKB | 1 | 1 | 24 | 1 | 4.2 | N/A |
| FAM166A | 1 | 1 | 24 | 1 | 4.2 | N/A |
| DIS3 | 1 | 1 | 24 | 1 | 4.2 | N/A |
| CTCF | 1 | 1 | 24 | 1 | 4.2 | N/A |
| C3orf70 | 1 | 1 | 24 | 1 | 4.2 | N/A |
| BCLAF1 | 1 | 1 | 24 | 1 | 4.2 | N/A |
| ALPK2 | 1 | 1 | 24 | 1 | 4.2 | N/A |
| NRAS | 1 | 1 | 65 | 2 | 3.1 | N/A |
| SMARCB1 | 1 | 1 | 60 | 1 | 1.7 | N/A |
| ABL | 1 | 1 | 65 | 1 | 1.5 | N/A |
| EGFR | 1 | 1 | 65 | 1 | 1.5 | N/A |
| MET | 1 | 1 | 65 | 1 | 1.5 | N/A |
| RET | 1 | 1 | 65 | 1 | 1.5 | N/A |
| Chromosome Region Studied | Event | Targeted Genes | Studies Identifying Alterations in the Gene | Number of PSCC Assessed | Number of PSCC with Gene Alteration | Overall Frequency (%) | Frequency Range (%) |
|---|---|---|---|---|---|---|---|
| Copy number alterations identified in more than one study | |||||||
| 8q24 | Gains | MYC | 2 | 80 | 26 | 32.5 | 18–75 |
| 7p12.1 to 11.2 | Gains | EGFR | 2 | 80 | 20 | 25.0 | 10–70 |
| Copy number alterations identified in one study | |||||||
| 14q32.33 | Amplifications | ADAM 6, KIAA0125, LINC00226, LINC00221 miR7641-2 | 1 | 20 | 20 | 100 | N/A |
| 2p12-p11.2 | Gains | REEP, CTNNA2, LRRTM1, ATOH8, DNAH6, FABP1, CD8A, CD8B, C2orf3, FAM176A, SUCCLG1, ELMOD3, USP39, VAMP8, FOXI3, FAM176A, SMYD1 | 1 | 20 | 20 | 100 | N/A |
| 10q26.13 | Gains | MGMT, EBF3, JAKMIP3, INPP5A, KNDC1, GLRX3, PPP2R2D, BNIP3, DPYSL4, LRRC27, ADAM8, PRAP1, PTER, PAOX, MTG1, CALY, SPRN, UTF1 | 1 | 20 | 17 | 85.0 | N/A |
| 8p23.1 | Losses | MCPH1, SGK223, SOX7, GATA4, PINX1, TDH, FAM66A | 1 | 20 | 17 | 85.0 | N/A |
| 10q11.22 | Losses/deletions | ZNF488, GDF2, SYT15, MAPK8, RBP3 | 1 | 20 | 15 | 75.0 | N/A |
| 1p36.3 | Gains | VWA1, CCNL2, MIB2, ATAD3A, GNB1, HES5, TP73 | 1 | 20 | 15 | 75.0 | N/A |
| 14q11.2 | Losses/deletions | CHD8, TOX4, APEX1, SALL2 | 1 | 20 | 14 | 70.0 | N/A |
| 15q11.2-q13.3 | Gains | OCA2, CYFIP1, TRPM1, BCL8 | 1 | 20 | 13 | 65.0 | N/A |
| 8q11.1-q24.3 | Gains | TOX, WISP1, IL7, STK3, SOX17, RP1, MAFA | 1 | 20 | 13 | 65.0 | N/A |
| 10p11.23 | Deletions | Bmi1 | 1 | 35 | 22 | 62.9 | N/A |
| 1q43 | Gains | IRF2BP2, ARID4b, LYST, GGPS1, FMN2 | 1 | 20 | 12 | 60.0 | N/A |
| 7q21.11 | Gains | CD36, GNAT3, TMEM60, PHTF2 | 1 | 20 | 12 | 60.0 | N/A |
| 2p24.3 | Amplifications | MYCN | 1 | 35 | 20 | 57.1 | N/A |
| 15q11.1-q11.2 | Losses/deletions | BCL8, CYFIP1, NIPA1, NIPA2 | 1 | 20 | 11 | 55.0 | N/A |
| 17p13.1 | Deletions | TP53 | 1 | 35 | 19 | 54.3 | N/A |
| 8q24.3 | Amplifications | PTK2 (FAK) | 1 | 35 | 19 | 54.3 | N/A |
| 12q15 | Deletions | MDM2 | 1 | 35 | 18 | 51.4 | N/A |
| 22q11.21 | Gains | BID, CECR2, TBX1, GSC2, HIRA | 1 | 20 | 10 | 50.0 | N/A |
| 2p25.3-p11.1 | Gains | SOX11, REL, FOXI3, EGR4, SIX3, TLX2, BIRC6, CD8B | 1 | 20 | 10 | 50.0 | N/A |
| 3q26.1 | Gains | MECOM, SI, PDCD10 | 1 | 20 | 10 | 50.0 | N/A |
| 17q21.33 | Deletions | NGFR (p75NTR) | 1 | 35 | 17 | 48.6 | N/A |
| 15q26.2-q26.3 | Gains | CHD2, IGF1R, RGMA, MEF2A, PTER, SYNM | 1 | 20 | 9 | 45.0 | N/A |
| 4q13.2 | Losses | UGT2B4, STAP1, TMPRSS11D | 1 | 20 | 9 | 45.0 | N/A |
| 5q13.2 | Losses/deletions | SKP2, BRIX1, IL7R, GDNF, RAD1, BRIX1, SPEF2 | 1 | 20 | 9 | 45.0 | N/A |
| 7p21.3 | Gains | PHF14, COL281A, RPA3, ARL4A | 1 | 20 | 9 | 45.0 | N/A |
| 14q12 | Gains | REC8, TINF2, PRKD1, IL25, FOXG1 | 1 | 20 | 8 | 40.0 | N/A |
| 16p11.2-p11.1 | Gains | ZNF689, ZNF668, YPEL3, PYCARD, MAZ, IL27, CD19 | 1 | 20 | 8 | 40.0 | N/A |
| 1q21.2 | Losses | POLR3C, BCL9, PDE4DIP, TXNIP, CD160, ACP6 | 1 | 20 | 8 | 40.0 | N/A |
| 20q13.32-q13.33 | Gains | BIRC7, DIDO1, ZGPAT, CTCFL, GNAS, SPO11, SLC2A4RG, GATA5, TAF4, PTK6 | 1 | 20 | 8 | 40.0 | N/A |
| 9p21 | Gains | CDKNB, ACO1, TAF1L, TEK, IFT74, IFNK, TUSC1, MLLT3 | 1 | 20 | 8 | 40.0 | N/A |
| 1q23.1 | Amplifications | NTRK1(TRKA) | 1 | 35 | 13 | 37.1 | N/A |
| 2p16.3 | Gains | MSH2, MSH6, FOXN2, NRXN1, FSHR | 1 | 20 | 7 | 35.0 | N/A |
| 1p36.13 | Deletions | ZBTB17(Miz1) | 1 | 35 | 12 | 34.3 | N/A |
| 11q24-q25 | Gains | ST14, CDON, OPCML, BARX2, ETS1, ADAMTS15, PTER | 1 | 20 | 5 | 25.0 | N/A |
| 14q31-q31.3 | Gains | GPR65, STON2, FLRT2 | 1 | 20 | 5 | 25.0 | N/A |
| 18p11.31 -p11.21 | Gains | LAMA1, APCDD1, TGIF1, MC5R | 1 | 20 | 5 | 25.0 | N/A |
| 7p22.3-p11 | Gains | PMS2, ADAP1, FAM126A, TSPAN13, MAFK | 1 | 20 | 5 | 25.0 | N/A |
| Yp11.3-p11.2 | Gains | CD99, ZBED1, TSPY1 | 1 | 20 | 5 | 25.0 | N/A |
| 9p21.3 | Losses | CDKN2A | 1 | 60 | 13 | 21.6 | N/A |
| 14q23.3 | Amplifications | Max | 1 | 35 | 7 | 20.0 | N/A |
| 11q13.3 | Gains | CCND1 | 1 | 60 | 8 | 13.3 | N/A |
| 3q26.33 | Gains | SOX2 | 1 | 60 | 8 | 13.3 | N/A |
| 3q26.33 | Gains | ATP11B | 1 | 60 | 5 | 8.3 | N/A |
| 5p15.33 | Gains | TERT | 1 | 60 | 4 | 6.7 | N/A |
| 3q26.33 | Gains | DCUN1D1 | 1 | 60 | 3 | 5.0 | N/A |
| 10p14 | Losses | GATA3 | 1 | 60 | 2 | 3.3 | N/A |
| 11p13 | Gains | CD44 | 1 | 60 | 2 | 3.3 | N/A |
| 22q12.2 | Losses | NF2 | 1 | 60 | 2 | 3.3 | N/A |
| 3q26.32 | Gains | PIK3CA | 1 | 60 | 2 | 3.3 | N/A |
| 11q22.2 | Gains | BIRC3 | 1 | 60 | 1 | 1.7 | N/A |
| 12q14.1 | Gains | CDK4 | 1 | 60 | 1 | 1.7 | N/A |
| 20q11.21 | Gains | BCL2L1 | 1 | 60 | 1 | 1.7 | N/A |
| 4q31.3 | Losses | FBXW7 | 1 | 60 | 1 | 1.7 | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribera-Cortada, I.; Guerrero-Pineda, J.; Trias, I.; Veloza, L.; Garcia, A.; Marimon, L.; Diaz-Mercedes, S.; Alamo, J.R.; Rodrigo-Calvo, M.T.; Vega, N.; et al. Pathogenesis of Penile Squamous Cell Carcinoma: Molecular Update and Systematic Review. Int. J. Mol. Sci. 2022, 23, 251. https://doi.org/10.3390/ijms23010251
Ribera-Cortada I, Guerrero-Pineda J, Trias I, Veloza L, Garcia A, Marimon L, Diaz-Mercedes S, Alamo JR, Rodrigo-Calvo MT, Vega N, et al. Pathogenesis of Penile Squamous Cell Carcinoma: Molecular Update and Systematic Review. International Journal of Molecular Sciences. 2022; 23(1):251. https://doi.org/10.3390/ijms23010251
Chicago/Turabian StyleRibera-Cortada, Inmaculada, José Guerrero-Pineda, Isabel Trias, Luis Veloza, Adriana Garcia, Lorena Marimon, Sherley Diaz-Mercedes, José Ramon Alamo, Maria Teresa Rodrigo-Calvo, Naiara Vega, and et al. 2022. "Pathogenesis of Penile Squamous Cell Carcinoma: Molecular Update and Systematic Review" International Journal of Molecular Sciences 23, no. 1: 251. https://doi.org/10.3390/ijms23010251